Achilles tendinopathy and tendon rupture
- Authors:
- Karen L Maughan, MD
- Blake Reid Boggess, DO, FAAFP
- Section Editor:
- Karl B Fields, MD
- Deputy Editor:
- Jonathan Grayzel, MD, FAAEM
INTRODUCTIONPain of the Achilles tendon commonly affects both competitive and recreational athletes as well as the sedentary. The largest tendon in the body, the Achilles tendon, endures strain and risks rupture from running, jumping, and sudden acceleration or deceleration. Overuse, vascular diseases, neuropathy, and rheumatologic diseases may cause tendon degeneration. The hallmarks of Achilles tendon problems seem to be damaged, weak, inelastic tissue.
This topic review will discuss the mechanism, diagnosis, and management of Achilles tendinopathy and tendon rupture. A general discussion of treatments for tendinopathy is provided separately. (See “Overview of the management of overuse (persistent) tendinopathy”.)
TERMINOLOGYTendonitis, tendinosis, tendinopathy, paratendinitis, enthesopathy, and insertional tendonitis are among the terms used to characterize acute or chronic tendon pain. The common term tendonitis is confusing because inflammation is often not seen on histopathology. Throughout this review, we will use the term tendinopathy to refer to acute and chronic pain associated with an Achilles tendon injury other than tendon tear or rupture. (See “Overview of overuse (persistent) tendinopathy”, section on ‘Pathology and terminology’.)
EPIDEMIOLOGY AND RISK FACTORSAchilles tendinopathy affects competitive and recreational athletes as well as people who are not active [1]. The incidence of Achilles tendon rupture in the general population is approximately 5 to 10 per 100,000, but may be higher in some regions and populations, and is increasing overall [2-5]. Over 80 percent of ruptures occur during recreational sports. Approximately 10 percent of patients who sustain an Achilles tendon rupture had preexisting Achilles tendon problems [6].
Observational data suggest that competitive athletes have a lifetime incidence of Achilles tendinopathy of 24 percent, with 18 percent sustained by athletes younger than 45 years [7]. Tendon rupture occurs in 8.3 percent of competitive athletes. Among competitive runners, the lifetime incidence of Achilles tendinopathy may be as high as 40 to 50 percent.
Competitive athletes with a high lifetime incidence of tendon rupture include sprinters (18 percent), decathletes (17 percent), soccer players (17 percent), track and field jumpers (12 percent), basketball players (12 percent), and ice hockey players (9 percent) [7]. Achilles tendinopathy in recreational runners, although less likely to involve rupture, accounts for 6 to 17 percent of all running injuries [8]. Military recruits develop tendinopathy at a rate of 6.8 percent [9].
Cold weather training is associated with higher rates of tendon pain [9]. Foot misalignment, poor running mechanics (excessive supination, inadequate dorsiflexion), inappropriate footwear, and leg length discrepancy are associated with tendon pain [10,11].
Age, male gender, and obesity are risk factors for Achilles tendon problems (table 1) [12]. The peak age for rupture is 30 to 40 years for both men and women; this may be when degenerative changes and occasional high stress from sports coincide. Rupture is four to five times more common in men than women [2]. As participation in recreational sports has increased over the past 50 years, so has the rate of tendon rupture [13].
Fluoroquinolone antibiotics are rarely associated with Achilles tendinopathy or tendon rupture. A study of 46,776 patients treated with fluoroquinolones found 3.2 cases of tendon problems for every 1000 years of exposure. Symptoms typically developed within one week of initiating treatment (median 6 days; range 1 to 510 days) [14], and the vast majority (85 to 93 percent) of patients reported symptoms within one month [15]. Among symptomatic patients without tendon rupture, most report recovery within two months of discontinuing the fluoroquinolone antibiotic, but in 26 percent, pain and disability persisted at long-term follow-up (timeframe not specified) [14]. According to a large case-control study, the incidence of tendon rupture associated with fluoroquinolone therapy is estimated at 12 per 100,000 treatment episodes (odds ratio [OR] 1.3; 95% CI 1.0-1.8) [16,17]. The risk of suffering an Achilles tendon rupture is increased threefold during the first 90 days among patients taking a fluoroquinolone for the first time. The mechanism remains unknown. Age older than 60 years and concurrent use of systemic glucocorticoids further increases the risk of Achilles problems [18-21]. Past fluoroquinolone use does not appear to confer future risk. (See “Fluoroquinolones”, section on ‘Tendinopathy and tendon rupture’.)
Oral glucocorticoids alone increase the risk of tendinopathy, although studies estimating the precise risk in primary care populations are lacking. Local glucocorticoid injection causes tendon damage in animal models, and there are case reports in humans of tendon rupture following glucocorticoid injection [22].
In women, hypertension is associated with Achilles tendinopathy [12]. Other diseases associated with tendinopathy include psoriasis and ankylosing spondylosis [23]. Heel pain is rarely the presenting symptom in patients with these systemic diseases [24].
CLINICAL ANATOMYThe soleus and gastrocnemius muscles converge to form the Achilles tendon, which inserts posteriorly on the calcaneus (figure 1 and figure 2). Contraction of these muscles, along with the actions of the tibialis posterior and peroneus longus and brevis, causes the foot to plantar flex. The subcutaneous and subtendinous (or retrocalcaneal) calcaneal bursae cushion the insertion area anteriorly and posteriorly. Most pain and tendon ruptures occur where the blood supply of the gastrocnemius-soleus muscle complex is poorest, 2 to 6 cm above the insertion point. A peritendinous sheath of connective tissue allows the tendon to slide relative to surrounding tissue.
MECHANISM OF INJURY AND PATHOPHYSIOLOGYAcute Achilles tendon pain generally develops when athletes abruptly increase their activity (eg, runners who start training for a marathon). Chronic tendon pain (>3 months) may result from sustained stress, poor running mechanics (eg, supination, heel misalignment), or improper footwear [13,25]. Some experts claim a role for excessive pronation in Achilles tendinopathy among runners, but others dispute this.
Recurrent microtrauma causes degeneration of the Achilles tendon [13,26]. The relative hypovascularity of the tendon 2 to 6 cm from its insertion point may prevent adequate healing. Although inflammation is often not seen on histopathology, clinical signs similar to those seen with inflammation (such as swelling, warmth, and pain) may occur. Damaged tendons become calcified, thickened, inelastic, and fibrotic. Abnormal neovascularization of tissue may be seen on ultrasound. Aging and vascular disease decrease collagen density, break collagen cross-links, and reduce the elasticity of the tendon sheath and tendon itself. Rupture occurs when a sudden shear stress (eg, cutting during a basketball game) is applied to an already weakened or degenerative tendon. The pathophysiology of overuse (chronic) tendinopathy is discussed in greater detail separately. (See “Overview of overuse (persistent) tendinopathy”.)
DIFFERENTIAL DIAGNOSIS
Overview — Apart from Achilles tendinopathy, pain arising from the region between the posterior calcaneus and the gastrocnemius-soleus muscle complex may be caused by several other conditions (table 2). Ankle sprain is the most common misdiagnosis when tendon rupture is the actual cause of pain [27]. Differentiating the two can be difficult. In contrast to ankle sprains, where injury occurs with landing, symptom onset with tendon rupture generally occurs as the patient is pushing off with their foot. Do NOT assume rupture is absent because the patient can plantar-flex their ankle or walk. The tibialis posterior and peroneus longus provide significant strength in plantar flexion and compensate partially for a ruptured Achilles tendon. (See ‘Physical examination’ below and “Ankle sprain”.)
Calcaneal bursitis — Calcaneal bursitis (subcutaneous or subtendinous) typically occurs in middle-aged or older adult patients. Patients may complain of pain where the back of a hard shoe or a strap rubs against the heel at the Achilles tendon insertion point. Sports in which athletes wear hard-backed footwear or repeatedly strike their heels against walls (eg, indoor soccer, hockey) may cause bursitis. Bursitis generally resolves with basic measures: heel lifts or posterior padding, avoiding bothersome footwear, rest, ice, and nonsteroidal antiinflammatory drugs (NSAIDs). Heel pain may also stem from an injury or strain at the Achilles tendon insertion (ie, enthesopathy). (See “Bursitis: An overview of clinical manifestations, diagnosis, and management”.)
Calcaneal apophysitis — Calcaneal apophysitis (ie, Sever disease) is an overuse injury in young athletes aged 8 to 15 years. Patients with calcaneal apophysitis have activity-related pain in the posterior aspect of the heel, which may be unilateral or bilateral. Tenderness is localized to the calcaneal apophysis, usually 1 to 2 cm distal to the Achilles tendon insertion. Symptoms generally resolve within three to six weeks with conservative treatment. (See “Heel pain in the active child or skeletally immature adolescent: Overview of causes”, section on ‘Calcaneal apophysitis (Sever disease)’.)
CLINICAL PRESENTATION
Tendinopathy — Patients with Achilles tendinopathy typically complain of pain or stiffness 2 to 6 cm above the posterior calcaneus. They are likely to be casual or competitive athletes who have increased their training regimen beyond their tendon’s ability to heal the microtrauma from repetitive stress, or who have been training rigorously for a long time. A history of excessive supination, increased speed work or hill training, or improper or worn out footwear may be found.
The pain is usually described as burning. The pain is worse with activity and relieved after a period of rest.
Tendon rupture — Tendon rupture occurs when sudden forces are exerted upon the Achilles tendon during strenuous physical activities that involve sudden pivoting on a foot or rapid acceleration (eg, stop and go sports such as tennis, basketball, or softball). Many patients feel as if they were struck violently in the back of the ankle. Some hear a “pop” and experience severe acute pain, although the absence of pain does not rule out rupture. As an example, a small case series found that one-third of patients with tendon rupture did not report pain [27]. In contrast to ankle sprains, where injury occurs with landing, symptom onset with tendon rupture generally occurs as the patient is pushing off with their foot.
PHYSICAL EXAMINATION
General evaluation — Examination of the Achilles tendon is usually straightforward because the tendon is easily identified and palpated. However, potential pitfalls exist (table 3). Of note, a sizable minority of patients with complete tendon rupture are able to ambulate.
Patients should be examined lying prone with their feet hanging off the end of the examination table. Inspect the region of the Achilles tendon for bruising (blood tracking beneath the malleolus suggests fracture, sprain, or tendon rupture), swelling, and foot misalignment. Assess patients for signs of peripheral artery disease, such as decreased pulsations, decreased capillary refill in the heel or toes, loss of hair, increased skin pigmentation, or edema.
Palpate the Achilles tendon for tenderness, thickening, or a defect, recognizing that edema or a hematoma may mask such a defect. Palpation has a sensitivity of approximately 73 percent and specificity of 89 percent in detecting a partial tendon tear [28]. Comparison to the unaffected side is useful.
Patients with tendinopathy typically have localized tenderness 2 to 6 cm proximal to the insertion of the tendon (picture 1). By comparison, tenderness around the insertion point near the heel suggests either subcutaneous calcaneal bursitis or enthesopathy (pathology of tendon at its insertion) [29]. Warmth and tenderness localized to the soft tissue anterior to the area where the Achilles inserts suggests subcutaneous bursitis, although this condition is uncommon. Focal tenderness of the tendon itself in the area where it inserts suggests enthesopathy.
The tendon should be palpated as the patient dorsi-flexes and plantar-flexes the foot, as well as when the ankle is stationary in a neutral position. The presence of crepitus with motion suggests tendinopathy.
Isolating the subtendinous bursa (ie, retrocalcaneal bursa) and palpating it for tenderness may identify bursitis. We perform this examination as follows: Grasp the Achilles tendon with the fingers of one hand and move the tendon side to side. Bursitis should not cause pain when only the tendon is palpated. Next, with the index finger on the opposite hand, apply gentle pressure deep to the tendon. Continue to grasp the tendon with the other hand to be certain you are palpating the bursa and not the tendon. Local warmth and tenderness deep to the tendon with light pressure suggests the subtendinous (or retrocalcaneal) bursa is inflamed.
Examine the patient’s footwear, looking for signs of excessive breakdown (eg, disproportionate wear on the inner or outer edge) or other evidence of poor running mechanics. Examine the architecture of the patient’s foot. The presence of flat feet (pes planus), heel malalignment, high arches (pes cavus), or leg length discrepancy can contribute to poor running mechanics [30]. If possible, assess the patient’s gait or running stride looking for abnormalities or asymmetry.
Special tests — The calf squeeze or Thompson test provides an accurate means for detecting complete Achilles tendon rupture (picture 2). To perform the test, the patient either lies prone with their feet hanging off the end of the examination table, or kneels on a chair. The clinician squeezes the gastrocnemius muscle belly while watching for plantar flexion. The absence of plantar flexion when squeezing the gastrocnemius muscle marks a positive test indicative of rupture.
The calf squeeze test is a more reliable indication of tendon rupture than the inability to plantar flex, since patients may be able to plantar flex the foot using accessory muscles (eg, tibialis posterior, peroneals). Achilles tendon ruptures can be missed at the initial visit because the clinician was falsely reassured by the patient’s ability to plantar flex or walk.
In a series of 174 patients with a clinical diagnosis of unilateral complete Achilles tendon tear and 28 patients with unilateral suspected but no actual Achilles tendon tear, the Thompson test had a sensitivity of 96 percent and a specificity of 93 percent, using magnetic resonance imaging (MRI) or ultrasound as a gold standard [28]. A negative test can miss up to 10 percent of ruptures (assuming a 75 percent pretest probability of rupture). Thus, confirmatory testing such as diagnostic ultrasound or MRI is useful when the Thompson test is negative but clinical suspicion remains high.
The Matles test is another means of assessing Achilles tendon rupture. To perform the test, the patient lies prone with knees flexed to 90 degrees. Observe whether the affected foot is dorsiflexed or neutral (both are abnormal) compared with the uninjured side, where the foot should appear plantar-flexed. The sensitivity and specificity of the Matles test was 88 percent and 85 percent, respectively, in the above study [28].
DIAGNOSTIC IMAGINGAchilles tendinopathy (without rupture) is a clinical diagnosis. Imaging is generally not necessary except to rule out other conditions, such as a stress fracture or tendon rupture.
Plain radiographs are generally unhelpful in the assessment of Achilles tendon pathology but may reveal a heel spur or bony bump (called a Haglund’s deformity or “pump bump”) consistent with both tendinopathy and calcaneal bursitis.
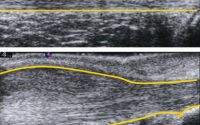
Ultrasound imaging is increasingly used to assess tendon appearance and function. Ultrasound may reveal normal tendon, tendon thickening, or signs of more significant tendon pathology, such as neovessels, hypoechogenicity, disordered fibers, tissue gaps, and fluid (image 1) [31]. Ultrasound can also help to distinguish between Achilles tendon injury and other pathology (image 2).
Achilles tendon rupture may be diagnosed solely by clinical examination, but ultrasound enables rapid bedside confirmation of the diagnosis [28]. Although published data are limited, in experienced hands ultrasound appears to be an accurate tool for diagnosing Achilles tendon tear and distinguishing between partial and complete tears. As an example, ultrasound was reported to have 100 percent sensitivity, 83 percent specificity, and 92 percent accuracy for distinguishing between partial and full thickness Achilles tendon tears, using surgical findings as the gold standard [32]. In addition, dynamic ultrasound can demonstrate whether tendon fragments come into contact during active plantar flexion or separate further during passive dorsiflexion. Visualized lack of continuity of tendon fibers is an indication for surgical repair.
Magnetic resonance imaging (MRI) is often used to assess musculoskeletal complaints and is the study of choice when tendon rupture is suspected and high-quality diagnostic ultrasound is unavailable. MRI provides greater anatomic detail and greater accuracy in detecting partial Achilles tendon tears [33]. With tendinopathy, MRI may demonstrate an increased T2-weighted signal in the tendon or an increased tendon diameter [34]. In addition, MRI may reveal alternative explanations for patient symptoms, such as enlarged calcaneal bursae.
Neither ultrasound nor MRI findings appear to correlate closely with clinically significant chronic Achilles tendinopathy. In one small prospective study, ultrasound detected abnormal morphology in 37 of 57 symptomatic Achilles tendons, while MRI detected abnormalities in 19 of 34 (MRI was performed in a subset of 25 consecutive patients) [35]. Better baseline MRI appearance was associated with a successful return to sport and symptomatic benefit after 12 months, but baseline ultrasound findings were not. Further study of these diagnostic tests is needed to determine their appropriate role in the management of Achilles tendinopathy.
ADDITIONAL ULTRASOUND RESOURCESInstructional videos demonstrating proper performance of the ultrasound examination of the ankle, including the Achilles tendon, and related pathology can be found at the website of the American Medical Society for Sports Medicine: sports US ankle-foot pathology. Registration must be completed to access these videos, but no fee is required.
INDICATIONS FOR REFERRALAll complete tendon ruptures merit referral for orthopedic consultation. The patient should be evaluated by the surgeon within approximately a day or two of the injury. It is best to discuss the case with the consulting orthopedist as soon as the injury is diagnosed.
Partial tendon tears and chronic tendinopathy that fail to improve with three to six months of conservative treatment may benefit from consultation with a specialized runners’ clinic, physical medicine and rehabilitation specialist, physical therapist, or orthopedic surgeon [36]. (See ‘Tendon rupture’ below.)
TREATMENT
Acute tendinopathy — Treatment of acute Achilles tendinopathy generally consists of the following:
●Avoid aggravating activities
●Apply ice when symptomatic
●Take a short course (7 to 10 days) of nonsteroidal antiinflammatory drugs (NSAIDs)
●Support the Achilles with a heel lift or elastic bandage or taping (picture 3) as needed
The goal of therapy is to relieve symptoms and enable a return to activity. Although the approach described here appears reasonable, there is little evidence to support it.
A systematic review of treatments for “Achilles tendinitis” published in 2001 identified three small controlled trials comparing oral NSAIDs to placebo [37]. Although there is no compelling evidence that NSAIDs enable patients to return to full activity sooner, these drugs are a reasonable choice for short-term pain relief in patients with acute Achilles tendinopathy. The role of oral and topical NSAIDs in the treatment of tendinopathy is reviewed separately. (See “Overview of the management of overuse (persistent) tendinopathy”, section on ‘Antiinflammatory medications’.)
A subsequent systematic review of studies looking at the effect of various injections, including glucocorticoids, for the treatment of Achilles tendinopathy found that the studies were of low quality overall, but the results suggest little if any benefit from such therapy [38]. This conclusion is consistent with studies of glucocorticoid injection for other tendinopathies. Glucocorticoid injection may provide short-term symptom relief in some cases. There are case reports of Achilles tendon rupture after glucocorticoid injection in patients with chronic tendinopathy [22]. (See “Overview of the management of overuse (persistent) tendinopathy”, section on ‘Glucocorticoids’.)
Once acute healing has begun, most patients begin some form of rehabilitation. Basic therapy regimens, including such interventions as physical therapy, deep-friction tissue release, and ultrasound, may reduce symptoms over several weeks [39]. Patients should perform an adequate warm-up before and stretch following inciting activities, once these are resumed. Rehabilitation for chronic Achilles tendinopathy and prevention strategies is discussed below. (See ‘Chronic tendinopathy’ below and ‘Prevention’ below.)
Small randomized trials have found no benefit from low-dose heparin injections or heel pads, but such pads may reduce pain from calcaneal bursitis [37].
Chronic tendinopathy — Chronic Achilles tendinopathy exists when pain persists beyond three months. In addition to the basic interventions for acute exacerbations described above, the treatment of chronic midportion Achilles tendon pain should include a rehabilitation program that emphasizes resistance exercises using heavy loads. A general discussion of treatments for tendinopathy is provided separately. (See “Overview of the management of overuse (persistent) tendinopathy”.)
Rehabilitation using resistance exercise — We suggest that patients with chronic mid-portion Achilles tendinopathy be treated with a rehabilitation program that emphasizes resistance exercises using heavy loads, such as weighted heel raises. Programs that emphasize the eccentric portion of exercise movements or both the eccentric and concentric movements may be used. Tables describing a heavy slow resistance rehabilitation program (emphasizes both concentric and eccentric movement) (table 4) and an eccentric exercise rehabilitation program (table 5) are provided [8,40].
Concentric exercise involves a muscle shortening while working against a load; eccentric exercise involves a muscle lengthening while working against a load. As an example, when a person raises their body to the bar during a pull-up the biceps muscles are working concentrically, and when the person lowers their body to the ground the biceps muscles are working eccentrically.
Studies of rehabilitation programs for chronic mid-portion Achilles tendinopathy that emphasize the eccentric portions of resistance exercise using heavy loads have found this approach to be an effective non-surgical treatment [41]. Other research suggests that programs using heavy resistance exercise emphasizing both the concentric and eccentric movements produce comparable outcomes [40,41]. Ultrasound examinations performed during the long-term follow-up of patients who participated in rehabilitation programs involving heavy resistance training of either type (eccentric or combined concentric/eccentric loading) show normalization of tendon tissue.
Patients may perform other regular exercise while participating in either type of rehabilitation program, provided that the activities do not exacerbate symptoms. Mild discomfort is permissible.
Eccentric exercise training — Small controlled trials and uncontrolled studies have found that eccentric exercise using heavy loads and involving the gastrocnemius and soleus muscles reduces pain at 12 weeks and long-term follow-up (two to five years), and shortens the time needed to return to sports [8,42-45]. A systematic review found there was higher-quality evidence supporting the use of eccentric exercise than alternative treatments for midportion (ie, NOT insertional) Achilles tendinopathy [46]. It is not known whether eccentric exercise prevents tendon injury or chronic tendinopathy in runners or other athletes. A table describing the most rigorously studied eccentric training rehabilitation protocol is provided (table 5) [8]. (See ‘Prevention’ below.)
Heavy slow resistance training — According to the results of a well-performed, single-blinded randomized trial involving 58 patients with chronic Achilles tendinopathy, heavy slow resistance training emphasizing both the concentric and eccentric portions of the exercises selected produced the same improvements in symptoms, function, and tissue appearance on ultrasound achieved by patients following a training program that emphasized only the eccentric portion of exercises [40]. The improvements were sustained at one-year follow-up. Of note, patient compliance was significantly better among patients performing the heavy slow resistance rehabilitation (92 versus 78 percent in the eccentric training group). This improved compliance may have been related to the time required, which was 107 minutes/week for the heavy slow resistance training and 308 minutes/week for the eccentric training. The training program used in the study is summarized in the attached table (table 4).
Other interventions — Various treatments have been prescribed for chronic Achilles pain. According to a systematic review, high-quality evidence supporting these interventions is lacking [46]. Some are suggested as adjuncts to eccentric exercise:
●In a small randomized trial sponsored by the manufacturer of the AirHeel brace, use of the brace improved symptoms and function in patients with chronic Achilles tendinopathy [47]. The results did not differ between patients managed with the AirHeel brace or eccentric rehabilitation.
●Heel lifts, arch supports, orthotics, and running shoes that are stable and prevent over-supination are commonly prescribed, but studies supporting these interventions are limited and no benefit has been demonstrated [48,49]. Night splinting is not beneficial [50].
●Low-level laser therapy may be a useful adjunct to eccentric exercise, reducing pain during activity, according to small randomized trials [51].
●Adjunct treatment with platelet-rich plasma or autologous blood injection in patients provided no added benefit in patients treated with eccentric exercise rehabilitation, according to small randomized trials [52-54].
●Dry needling is used by some clinicians to treat Achilles tendinopathy. This involves repeated puncture of the tendon at the site of pain using a small needle with the intent of stimulating an inflammatory response, formulation of granulation tissue, ultimately causing tendon healing. (See “Overview of the management of overuse (persistent) tendinopathy”.)
●Ultrasound-guided, high-volume injection into the paratenon has been used in the hope of reducing pain by disrupting abnormal blood vessels and nerves. Preliminary studies suggest benefit, including earlier return to sport, but further study is needed [55-57].
●Kinesiotape (elastic therapeutic skin tape) has been used to treat Achilles tendinopathy, but evidence about its effectiveness is limited [58].
Tendon rupture
Initial care — Initial management of Achilles tendon rupture consists of ice applied to the area, analgesics (acetaminophen and/or NSAIDs are generally sufficient), rest (ie, non-weightbearing with crutches), immobilization with the ankle in some plantar flexion (generally a splint is used), and referral to an orthopedic surgeon.
Complete tendon rupture — Surgical consultation should be obtained for all complete Achilles tendon ruptures. The efficacy of surgery was evaluated in a systematic review of 12 randomized and quasi-randomized trials in which the following findings were noted [59]:
●Surgical repair reduced the risk of repeat tendon rupture compared with nonoperative management (12/240 [5 percent] versus 30/249 [12 percent]; risk ratio [RR] 0.41, 95% CI 0.21-0.77).
●Pooled results indicate that complications other than rerupture were reported more often in the surgically treated group, although this was not statistically significant when using the random-effects model (70/240 [29.2 percent] versus 20/249 [8 percent]; RR 4.81, 95% CI 0.78-29.56). These complications included infection, abnormal sensation (sural nerve injury), adhesions, and deep vein thrombosis.
●Although disparate outcome measures prevented the authors from pooling data, all studies but one found no significant difference in the percentage of patients treated surgically or nonoperatively who were able to return to their preinjury level of sporting activity.
●Four studies included in the review reported that percutaneous surgical repair reduced postoperative wound infections compared with open repair (0/68 versus 12/66; RR 9.32, 95% CI 1.77-49.16), without affecting rerupture rates. There was no significant difference in the rates of other complications.
●Assessments of recuperation time and patient satisfaction varied among studies and no clear conclusions could be drawn.
A subsequent meta-analysis of seven randomized trials reported similar results [60]. The rerupture rate among surgical patients in this review was 3.6 versus 8.8 percent among patients managed nonoperatively (OR 0.425; 95% CI 0.222-0.815). Several randomized trials published after both meta-analyses report consistent findings [61]. In addition, one small randomized trial reported greater calf muscle strength in patients treated surgically [62].
Despite the lower rerupture rates among surgical patients reported in these systematic reviews, the authors of several studies have questioned the preference for surgical repair when managing ruptured Achilles tendons [63-67]:
●In a controlled trial, 144 patients with acute Achilles tendon rupture were randomly assigned to operative or nonoperative treatment, with both groups also undergoing accelerated rehabilitation including early weightbearing and early range of motion exercises [64]. Although rerupture rates were comparable (2/72 patients in the operative group versus 3/72 in the nonoperative group), soft tissue complications (eg, infection) occurred more often among patients treated surgically (13/72 [18 percent] versus 6/72 [8 percent]). Other important clinical outcomes, including strength, motion, and overall function, were similar in both groups at one- and two-year follow-up.
●In a similar trial, 42 patients with acute Achilles tendon rupture were randomly assigned to surgery or no surgery, while treatment for both groups included early motion controlled in a removable orthosis, progressing to full weightbearing at eight weeks [65]. No differences in complications and a similar low number of re-ruptures were reported for both groups.
●In a long-term observational study not considered in either systematic review, 945 consecutive patients with both acute and delayed Achilles tendon rupture were managed with a nonsurgical approach using a structured functional rehabilitation protocol [63]. Patients were placed initially in a non-weightbearing cast with the foot in equinus position (plantar flexion), then transitioned to a pneumatic walker with elevated heels (elevation was gradually reduced biweekly), and finally received physical therapy to improve gait, strength, and mobility. Among patients treated with this protocol, rerupture rates were reported to be low (2.8 percent in the acute tendon rupture group; 2.7 percent in the delayed rupture group) regardless of the activities that they resumed.
The findings of these studies suggest that a nonoperative protocol using accelerated functional rehabilitation may avoid the major complications of surgical management without increasing the risk of rerupture [66]. If additional randomized trials replicate the findings of these studies, the appropriate role of surgical and nonsurgical management will need to be reconsidered.
For patients treated with surgery, two to three months off from work that requires ambulation is generally required. Athletes typically return to sports by three to six months, once they have regained adequate strength and mobility. However, additional time is often required to achieve full function [68]. According to a systematic review of 10 studies involving 570 patients, the combination of early ankle mobility exercises and early weightbearing was associated with better functional outcomes without differences in major complications compared with the conventional approach to postoperative immobilization [69].
Non-athletes and older patients may forego surgery and elect to be treated with immobilization using a plantar flexion short leg cast or a functional brace with a heel lift for six to eight weeks. These patients should be informed of the greater risk of repeat rupture. Ideally, casting should be performed within 48 hours of injury.
For patients who are found to have ruptured their Achilles tendon many weeks or months prior to diagnosis, immobilization with a brace followed by physical therapy is a reasonable management approach.
Partial tendon rupture — The clinical diagnosis of partial Achilles tendon tear or rupture is imperfect, and studies to determine optimal management are lacking. The increasing use of ultrasound and magnetic resonance imaging (MRI) may improve this situation. It remains unclear whether surgery or conservative management leads to better outcomes [70,71]. We treat most cases of partial Achilles tear nonsurgically, as we would chronic tendinopathy. (See ‘Chronic tendinopathy’ above.)
Partial tears can be painful. To reduce discomfort, initial management may include immobilization in a controlled ankle motion (CAM) boot (picture 4). Physical therapy or home exercises are needed to prevent the loss of motion and strength that can result from immobilization.
FOLLOW-UP CAREApproximately 80 percent of athletes return to play following rupture of their Achilles tendon [72]. Prevention of reinjury is central to follow-up care. Ten percent of Achilles tendon ruptures occur in previously injured tendons. Prevention of Achilles tendon injury is discussed immediately below.
Although no studies demonstrate the benefit of eccentric exercise in the prevention of acute Achilles tendon injury, we suggest that patients continue to perform these exercises once rehabilitation has been completed and symptoms have resolved. We believe this may be of particular benefit to athletes embarking upon a more intense training regimen. (See ‘Chronic tendinopathy’ above.)
Some patients treated for chronic Achilles tendinopathy have persistent symptoms, but it is unclear whether this is true of patients who complete a properly designed rehabilitation program emphasizing heavy resistance exercise. Patients who do not fully recover may experience reinjury [73].
PREVENTION
General measures — Several interventions may reduce the risk of developing new or recurrent Achilles tendinopathy, and other injuries of the lower extremity. Such interventions are discussed in detail separately. Interventions and studies of special relevance to preventing tendinopathy and tendon rupture of the Achilles are described below. (See “Overview of running injuries of the lower extremity”, section on ‘Training suggestions to reduce injury risk’.)
Before engaging in any vigorous exercise, it is important to perform an appropriate dynamic warm-up. Although few studies have assessed the Achilles tendon specifically in this regard, the findings of a prospective, observational study of infantry recruits suggest that performing such a warm-up and avoiding cold-weather training reduces the risk of Achilles tendinopathy [9]. Additional support may be helpful for some patients as they resume activity (picture 3).
Clinical studies evaluating the impact of stretching specifically upon Achilles tendinopathy are lacking. Nevertheless, many clinicians believe imbalances in muscle strength or flexibility predispose some athletes to injury. We believe it is reasonable to include stretching following exercise or a warm-up as part of an Achilles injury prevention regimen. Typical techniques include stretching the gastrocnemius and soleus muscles while bracing one’s hands against a wall. Stretches are performed both with the knee bent and straight. The stretch can be performed by standing on the edge of a step and letting the heel descend gradually, or by dorsiflexing the foot using a stretch band. It may be helpful for patients to undergo assessment by an athletic trainer, physical therapist, or sports medicine specialist to identify imbalances in flexibility or strength and to receive instruction in appropriate training techniques.
Although high body mass index (BMI) is associated with tendon problems, no studies clearly show that weight loss prevents such problems. Nevertheless, common sense suggests that obese patients should try to lose weight in order to reduce strain on the lower extremity, among many other health benefits. (See “Obesity in adults: Overview of management” and “Overweight and obesity in adults: Health consequences”.)
Measures for patients on fluoroquinolones — The risk of fluoroquinolone-associated tendon problems is low. However, for athletes or highly active patients who require fluoroquinolone treatment, it is reasonable to take precautions to reduce the risk of Achilles tendinopathy or tendon rupture. High-quality evidence to determine what measures are most effective is lacking, but the following steps are reasonable [74]:
●Beginning with the first fluoroquinolone dose, athletes should reduce their training volume and intensity and maintain these reductions throughout the course of antibiotics. No high-intensity training or ballistic activities (eg, sprinting, jumping, full speed scrimmages or competition) are permitted until two to four weeks after the completion of fluoroquinolone therapy.
●Runners should decrease total mileage to 60 percent of normal training volume for the first seven days of therapy, and hill and speed interval training should be avoided. Runners who remain free of symptoms two weeks after the completion of therapy may increase mileage by 10 percent per week but should not implement speed or hill training for two additional weeks. If they choose to race during this time they should be informed of the relatively higher risk of Achilles rupture.
●Athletes who participate in field sports (eg, soccer, football) or other multidirectional activities (eg, tennis) that increase the risk of Achilles injury may choose to resume normal activity and competition two to four weeks after the completion of fluoroquinolone therapy. However, it is best to increase activity gradually, and athletes who resume full activity sooner than four weeks should be informed of the higher relative risk of Achilles rupture.
●Athletes who have no symptoms during therapy and complete the full course of the antibiotic can begin a graduated return to full activity as described above but should monitor themselves closely for any musculoskeletal symptoms at or around the Achilles tendon. They should cease all athletic activity should symptoms develop during this period and be assessed by a knowledgeable clinician. Assuming there is no injury, they may resume a graduated return to full activity once symptoms resolve.
●Athletes who develop symptoms or tenderness around the Achilles while taking a fluoroquinolone antibiotic or in the first three to six months after beginning this treatment merit objective evaluation, preferably with musculoskeletal ultrasound to assess for findings of tendinopathy or other injury. Individuals with findings suggesting tendinopathy typically require an eccentric exercise rehabilitation program and possibly adjunctive therapy. Their return to play depends upon clinical response and averages 6 to 12 weeks. (See ‘Diagnostic imaging’ above and ‘Rehabilitation using resistance exercise’ above.)
SOCIETY GUIDELINE LINKSLinks to society and government-sponsored guidelines from selected countries and regions around the world are provided separately. (See “Society guideline links: Chronic tendon injury” and “Society guideline links: Achilles tendon rupture”.)
INFORMATION FOR PATIENTSUpToDate offers two types of patient education materials, “The Basics” and “Beyond the Basics.” The Basics patient education pieces are written in plain language, at the 5th to 6th grade reading level, and they answer the four or five key questions a patient might have about a given condition. These articles are best for patients who want a general overview and who prefer short, easy-to-read materials. Beyond the Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are written at the 10th to 12th grade reading level and are best for patients who want in-depth information and are comfortable with some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or e-mail these topics to your patients. (You can also locate patient education articles on a variety of subjects by searching on “patient info” and the keyword(s) of interest.)
●Basics topic (see “Patient education: Achilles tendinopathy (The Basics)”)
SUMMARY AND RECOMMENDATIONS
Presentation and diagnosis
●Acute tendon pain generally develops when athletes abruptly increase their training intensity. Chronic tendon pain (>3 months) may result from sustained stress, poor running mechanics, or improper footwear. Rupture occurs when a sudden shear stress is applied to an already weakened or degenerative tendon. (See ‘Epidemiology and risk factors’ above and ‘Mechanism of injury and pathophysiology’ above.)
●Pain arising from the region between the posterior calcaneus and the gastrocnemius-soleus muscle complex may be caused by a number of conditions (table 2). Ankle sprain is the most common misdiagnosis when tendon rupture is the actual cause of pain. Do not assume rupture is absent because the patient can plantar flex or walk. (See ‘Differential diagnosis’ above.)
●Patients with Achilles tendinopathy typically experience pain or stiffness 2 to 6 cm above the posterior calcaneus. They are likely to be casual or competitive athletes who have recently increased their training intensity. Pain increases with activity and diminishes with a period of rest. Tendon rupture occurs when sudden forces are exerted upon the Achilles during strenuous activities that involve sudden pivoting on a foot or rapid acceleration. Patients may hear a “pop” and experience severe acute pain, although the absence of pain does not rule out rupture. (See ‘Clinical presentation’ above.)
●Examination should include palpation of the Achilles tendon for tenderness, thickening, or a defect. Note that edema or a hematoma may mask a defect in the tendon. Patients with tendinopathy typically have localized tenderness 2 to 6 cm above the insertion point of the Achilles tendon. Pain at the insertion point suggests calcaneal bursitis or possibly enthesopathy. (See ‘Physical examination’ above.)
●The calf squeeze (ie, Thompson compression) test provides an accurate means for detecting complete Achilles tendon rupture (picture 2). A sizable minority of patients with complete tendon rupture are able to ambulate. (See ‘Physical examination’ above.)
●Achilles tendinopathy (without rupture) is a clinical diagnosis. Imaging is not generally necessary. Plain radiographs are generally unhelpful. Musculoskeletal ultrasound and magnetic resonance imaging (MRI) are accurate tests that can be used to aid in the diagnosis of Achilles tendon rupture. (See ‘Diagnostic imaging’ above.)
Treatment and prevention
●All complete tendon ruptures merit surgical consultation. Partial tendon tears and chronic tendinopathy that fail to improve with three to six months of conservative treatment may benefit from consultation with a specialized runners’ clinic, sports medicine specialist, physical therapist, or orthopedic surgeon. (See ‘Indications for referral’ above.)
●Acute Achilles tendinopathy is treated in standard fashion with rest, ice, and tendon support. For chronic midportion tendinopathy (>3 months symptoms), we suggest using a rehabilitation program that emphasizes resistance exercise using heavy loads (table 5) (Grade 2B). Exercise programs and other possible interventions for chronic Achilles tendinopathy are discussed in the text. (See ‘Acute tendinopathy’ above and ‘Chronic tendinopathy’ above.)
●We suggest that tendon rupture be treated with surgical repair (Grade 2A). This suggestion applies to active patients who place a high value on regaining preinjury levels of activity and are willing to accept a higher rate of treatment complications. Inactive patients and those unwilling to accept higher complication rates may opt for nonoperative management. Percutaneous surgical repair may reduce postoperative wound infection rates compared with open repair. Postoperatively and in patients who opt for nonsurgical management, early mobilization and functional rehabilitation improve function and quality of life without impairing healing. (See ‘Tendon rupture’above.)
●Several interventions may reduce the risk of developing lower extremity injuries, including Achilles tendinopathy. (See “Overview of running injuries of the lower extremity”, section on ‘Training suggestions to reduce injury risk’ and ‘Prevention’ above.)
ACKNOWLEDGMENTWe are saddened by the death of Peter Ham, MD, who passed away in January 2017. UpToDate wishes to acknowledge Dr. Ham’s past work as a co-author for this topic.
REFERENCES
- Alfredson H, Lorentzon R. Chronic Achilles tendinosis: recommendations for treatment and prevention. Sports Med 2000; 29:135.
- Leppilahti J, Puranen J, Orava S. Incidence of Achilles tendon rupture. Acta Orthop Scand 1996; 67:277.
- Suchak AA, Bostick G, Reid D, et al. The incidence of Achilles tendon ruptures in Edmonton, Canada. Foot Ankle Int 2005; 26:932.
- Huttunen TT, Kannus P, Rolf C, et al. Acute achilles tendon ruptures: incidence of injury and surgery in Sweden between 2001 and 2012. Am J Sports Med 2014; 42:2419.
- Sheth U, Wasserstein D, Jenkinson R, et al. The epidemiology and trends in management of acute Achilles tendon ruptures in Ontario, Canada: a population-based study of 27 607 patients. Bone Joint J 2017; 99-B:78.
- Leppilahti J, Orava S. Total Achilles tendon rupture. A review. Sports Med 1998; 25:79.
- Kujala UM, Sarna S, Kaprio J. Cumulative incidence of achilles tendon rupture and tendinopathy in male former elite athletes. Clin J Sport Med 2005; 15:133.
- Fahlström M, Jonsson P, Lorentzon R, Alfredson H. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc 2003; 11:327.
- Milgrom C, Finestone A, Zin D, et al. Cold weather training: a risk factor for Achilles paratendinitis among recruits. Foot Ankle Int 2003; 24:398.
- Järvinen TA, Kannus P, Paavola M, et al. Achilles tendon injuries. Curr Opin Rheumatol 2001; 13:150.
- Leppilahti J, Korpelainen R, Karpakka J, et al. Ruptures of the Achilles tendon: relationship to inequality in length of legs and to patterns in the foot and ankle. Foot Ankle Int 1998; 19:683.
- Holmes GB, Lin J. Etiologic factors associated with symptomatic achilles tendinopathy. Foot Ankle Int 2006; 27:952.
- Józsa L, Kvist M, Bálint BJ, et al. The role of recreational sport activity in Achilles tendon rupture. A clinical, pathoanatomical, and sociological study of 292 cases. Am J Sports Med 1989; 17:338.
- van der Linden PD, van Puijenbroek EP, Feenstra J, et al. Tendon disorders attributed to fluoroquinolones: a study on 42 spontaneous reports in the period 1988 to 1998. Arthritis Rheum 2001; 45:235.
- Akali AU, Niranjan NS. Management of bilateral Achilles tendon rupture associated with ciprofloxacin: a review and case presentation. J Plast Reconstr Aesthet Surg 2008; 61:830.
- Sode J, Obel N, Hallas J, Lassen A. Use of fluroquinolone and risk of Achilles tendon rupture: a population-based cohort study. Eur J Clin Pharmacol 2007; 63:499.
- Corrao G, Zambon A, Bertù L, et al. Evidence of tendinitis provoked by fluoroquinolone treatment: a case-control study. Drug Saf 2006; 29:889.
- van der Linden PD, Sturkenboom MC, Herings RM, et al. Fluoroquinolones and risk of Achilles tendon disorders: case-control study. BMJ 2002; 324:1306.
- Butler MW, Griffin JF, Quinlan WR, McDonnell TJ. Quinolone-associated tendonitis: a potential problem in COPD? Ir J Med Sci 2001; 170:198.
- van der Linden PD, Sturkenboom MC, Herings RM, et al. Increased risk of achilles tendon rupture with quinolone antibacterial use, especially in elderly patients taking oral corticosteroids. Arch Intern Med 2003; 163:1801.
- Wise BL, Peloquin C, Choi H, et al. Impact of age, sex, obesity, and steroid use on quinolone-associated tendon disorders. Am J Med 2012; 125:1228.e23.
- Kleinman M, Gross AE. Achilles tendon rupture following steroid injection. Report of three cases. J Bone Joint Surg Am 1983; 65:1345.
- Borman P, Koparal S, Babaoğlu S, Bodur H. Ultrasound detection of entheseal insertions in the foot of patients with spondyloarthropathy. Clin Rheumatol 2006; 25:373.
- Aldridge T. Diagnosing heel pain in adults. Am Fam Physician 2004; 70:332.
- Kaufman KR, Brodine SK, Shaffer RA, et al. The effect of foot structure and range of motion on musculoskeletal overuse injuries. Am J Sports Med 1999; 27:585.
- Kader D, Saxena A, Movin T, Maffulli N. Achilles tendinopathy: some aspects of basic science and clinical management. Br J Sports Med 2002; 36:239.
- Gravlee JR, Hatch RL, Galea AM. Achilles tendon rupture: a challenging diagnosis. J Am Board Fam Pract 2000; 13:371.
- Maffulli N. The clinical diagnosis of subcutaneous tear of the Achilles tendon. A prospective study in 174 patients. Am J Sports Med 1998; 26:266.
- Schepsis AA, Jones H, Haas AL. Achilles tendon disorders in athletes. Am J Sports Med 2002; 30:287.
- Johnston CA, Taunton JE, Lloyd-Smith DR, McKenzie DC. Preventing running injuries. Practical approach for family doctors. Can Fam Physician 2003; 49:1101.
- Archambault JM, Wiley JP, Bray RC, et al. Can sonography predict the outcome in patients with achillodynia? J Clin Ultrasound 1998; 26:335.
- Hartgerink P, Fessell DP, Jacobson JA, van Holsbeeck MT. Full- versus partial-thickness Achilles tendon tears: sonographic accuracy and characterization in 26 cases with surgical correlation. Radiology 2001; 220:406.
- Kayser R, Mahlfeld K, Heyde CE. Partial rupture of the proximal Achilles tendon: a differential diagnostic problem in ultrasound imaging. Br J Sports Med 2005; 39:838.
- Aström M, Gentz CF, Nilsson P, et al. Imaging in chronic achilles tendinopathy: a comparison of ultrasonography, magnetic resonance imaging and surgical findings in 27 histologically verified cases. Skeletal Radiol 1996; 25:615.
- Khan KM, Forster BB, Robinson J, et al. Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two year prospective study. Br J Sports Med 2003; 37:149.
- Maffulli N, Sharma P, Luscombe KL. Achilles tendinopathy: aetiology and management. J R Soc Med 2004; 97:472.
- McLauchlan GJ, Handoll HH. Interventions for treating acute and chronic Achilles tendinitis. Cochrane Database Syst Rev 2001; :CD000232.
- Kearney RS, Parsons N, Metcalfe D, Costa ML. Injection therapies for Achilles tendinopathy. Cochrane Database Syst Rev 2015; :CD010960.
- Mayer F, Hirschmüller A, Müller S, et al. Effects of short-term treatment strategies over 4 weeks in Achilles tendinopathy. Br J Sports Med 2007; 41:e6.
- Beyer R, Kongsgaard M, Hougs Kjær B, et al. Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial. Am J Sports Med 2015; 43:1704.
- Malliaras P, Barton CJ, Reeves ND, Langberg H. Achilles and patellar tendinopathy loading programmes : a systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Med 2013; 43:267.
- Roos EM, Engström M, Lagerquist A, Söderberg B. Clinical improvement after 6 weeks of eccentric exercise in patients with mid-portion Achilles tendinopathy — a randomized trial with 1-year follow-up. Scand J Med Sci Sports 2004; 14:286.
- Mafi N, Lorentzon R, Alfredson H. Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee Surg Sports Traumatol Arthrosc 2001; 9:42.
- Silbernagel KG, Thomeé R, Thomeé P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain–a randomised controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports 2001; 11:197.
- van der Plas A, de Jonge S, de Vos RJ, et al. A 5-year follow-up study of Alfredson’s heel-drop exercise programme in chronic midportion Achilles tendinopathy. Br J Sports Med 2012; 46:214.
- Magnussen RA, Dunn WR, Thomson AB. Nonoperative treatment of midportion Achilles tendinopathy: a systematic review. Clin J Sport Med 2009; 19:54.
- Petersen W, Welp R, Rosenbaum D. Chronic Achilles tendinopathy: a prospective randomized study comparing the therapeutic effect of eccentric training, the AirHeel brace, and a combination of both. Am J Sports Med 2007; 35:1659.
- Yeung EW, Yeung SS. Interventions for preventing lower limb soft-tissue injuries in runners. Cochrane Database Syst Rev 2001; :CD001256.
- Munteanu SE, Scott LA, Bonanno DR, et al. Effectiveness of customised foot orthoses for Achilles tendinopathy: a randomised controlled trial. Br J Sports Med 2015; 49:989.
- de Vos RJ, Weir A, Visser RJ, et al. The additional value of a night splint to eccentric exercises in chronic midportion Achilles tendinopathy: a randomised controlled trial. Br J Sports Med 2007; 41:e5.
- Stergioulas A, Stergioula M, Aarskog R, et al. Effects of low-level laser therapy and eccentric exercises in the treatment of recreational athletes with chronic achilles tendinopathy. Am J Sports Med 2008; 36:881.
- de Vos RJ, Weir A, van Schie HT, et al. Platelet-rich plasma injection for chronic Achilles tendinopathy: a randomized controlled trial. JAMA 2010; 303:144.
- de Jonge S, de Vos RJ, Weir A, et al. One-year follow-up of platelet-rich plasma treatment in chronic Achilles tendinopathy: a double-blind randomized placebo-controlled trial. Am J Sports Med 2011; 39:1623.
- Bell KJ, Fulcher ML, Rowlands DS, Kerse N. Impact of autologous blood injections in treatment of mid-portion Achilles tendinopathy: double blind randomised controlled trial. BMJ 2013; 346:f2310.
- Humphrey J, Chan O, Crisp T, et al. The short-term effects of high volume image guided injections in resistant non-insertional Achilles tendinopathy. J Sci Med Sport 2010; 13:295.
- Wheeler PC, Tattersall C. Novel Interventions for Recalcitrant Achilles Tendinopathy: Benefits Seen Following High-Volume Image-Guided Injection or Extracorporeal Shockwave Therapy-A Prospective Cohort Study. Clin J Sport Med 2018.
- Boesen AP, Hansen R, Boesen MI, et al. Effect of High-Volume Injection, Platelet-Rich Plasma, and Sham Treatment in Chronic Midportion Achilles Tendinopathy: A Randomized Double-Blinded Prospective Study. Am J Sports Med 2017; 45:2034.
- Parreira Pdo C, Costa Lda C, Hespanhol LC Jr, et al. Current evidence does not support the use of Kinesio Taping in clinical practice: a systematic review. J Physiother 2014; 60:31.
- Khan RJ, Carey Smith RL. Surgical interventions for treating acute Achilles tendon ruptures. Cochrane Database Syst Rev 2010; :CD003674.
- Wilkins R, Bisson LJ. Operative versus nonoperative management of acute Achilles tendon ruptures: a quantitative systematic review of randomized controlled trials. Am J Sports Med 2012; 40:2154.
- Olsson N, Silbernagel KG, Eriksson BI, et al. Stable surgical repair with accelerated rehabilitation versus nonsurgical treatment for acute Achilles tendon ruptures: a randomized controlled study. Am J Sports Med 2013; 41:2867.
- Lantto I, Heikkinen J, Flinkkila T, et al. A Prospective Randomized Trial Comparing Surgical and Nonsurgical Treatments of Acute Achilles Tendon Ruptures. Am J Sports Med 2016; 44:2406.
- Wallace RG, Heyes GJ, Michael AL. The non-operative functional management of patients with a rupture of the tendo Achillis leads to low rates of re-rupture. J Bone Joint Surg Br 2011; 93:1362.
- Willits K, Amendola A, Bryant D, et al. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am 2010; 92:2767.
- Twaddle BC, Poon P. Early motion for Achilles tendon ruptures: is surgery important? A randomized, prospective study. Am J Sports Med 2007; 35:2033.
- Soroceanu A, Sidhwa F, Aarabi S, et al. Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials. J Bone Joint Surg Am 2012; 94:2136.
- Nilsson-Helander K, Silbernagel KG, Thomeé R, et al. Acute achilles tendon rupture: a randomized, controlled study comparing surgical and nonsurgical treatments using validated outcome measures. Am J Sports Med 2010; 38:2186.
- Trofa DP, Miller JC, Jang ES, et al. Professional Athletes’ Return to Play and Performance After Operative Repair of an Achilles Tendon Rupture. Am J Sports Med 2017; 45:2864.
- McCormack R, Bovard J. Early functional rehabilitation or cast immobilisation for the postoperative management of acute Achilles tendon rupture? A systematic review and meta-analysis of randomised controlled trials. Br J Sports Med 2015; 49:1329.
- Robert Smigielski . Management of partial tears of the gastro-soleus complex. Clin Sports Med 2008; 27:219.
- Morberg P, Jerre R, Swärd L, Karlsson J. Long-term results after surgical management of partial Achilles tendon ruptures. Scand J Med Sci Sports 1997; 7:299.
- Zellers JA, Carmont MR, Grävare Silbernagel K. Return to play post-Achilles tendon rupture: a systematic review and meta-analysis of rate and measures of return to play. Br J Sports Med 2016.
- Silbernagel KG, Brorsson A, Lundberg M. The majority of patients with Achilles tendinopathy recover fully when treated with exercise alone: a 5-year follow-up. Am J Sports Med 2011; 39:607.
- Hall MM, Finnoff JT, Smith J. Musculoskeletal complications of fluoroquinolones: guidelines and precautions for usage in the athletic population. PM R 2011; 3:132.