
Acute Achilles tendon rupture
Youngseok Moon, Keun-Young Choi, Jae Hoon Ahn
Department of Orthopaedic Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
The incidence of Achilles tendon ruptures has risen with the increase in the level of sports activity of the average individual. An Achilles tendon rupture is generally diagnosed on the basis of clinical findings, sometimes in conjunction with ultrasound or magnetic resonance imaging tests. The treatment of Achilles tendon ruptures is broadly divided into surgical treatment and conservative treatment, and the gold standard treatment remains a controversial issue. The surgical treatment of Achilles tendon ruptures has been reported to be associated with a lower re-tear rate and thus has been the conventional choice of treatment, in particular the direct repair for its ability to restore muscle strength. But recently percutaneous repairs and minimally invasive methods have become more widespread. And the previously undervalued functional rehabilitation such as early weight-bearing and postoperative joint exercises has gained greater importance for their capacity to restore tendon function.
Keywords: Achilles tendon rupture; Conservative treatment; Direct repair; Functional rehabilitation.
INTRODUCTION
The Achilles tendon is the body’s thickest, largest, and strongest tendon. The Achilles tendon serves to attach the medial and lateral gastrocnemius muscles to the distal soleus muscle. And attached to its medial side is the plantaris tendon. Biomechanically, the Achilles tendon must endure 2–3 times more bodyweight during gait and up to 10 times more bodyweight during certain athletic activities [1].
The Achilles tendon rupture dates back to the lifetime of Hippocrates. It was first described in 1575 by Ambroise Paré and reported in the literature in 1633 [2]. The incidence of Achilles tendon ruptures has consistently increased from the 1980s, which is thought to be because of not only increased public awareness of health but also increased participation in active sports by the older generation who are more susceptible to these lesions, such as the middle-aged and the elderly [3]. This lesion is renowned for its debilitating consequences: around a third of athletes fail to return to pre-injury levels of sports [4].
Treatment for Achilles tendon ruptures can be divided into conservative treatment and surgical treatment such as open repairs, percutaneous repairs, and mini open repairs. In the past, there was greater preference for surgical treatment of Achilles tendon injuries, but with Lea and Smith’s report [5] on the conservative treatment for Achilles tendon ruptures, the use of conservative treatment has since increased.
ACHILLES TENDON RUPTURES
Epidemiology
The incidence of Achilles tendon ruptures was 4.7 per 100,000 in 1981, which steadily increased to 6 per 100,000 in 1994; to 22.1 per 100,000 in 1991; and to 32.6 per 1000,000 in 2002 [6-10]. The incidence of Achilles tendon ruptures in men has been reported to be 2–12 times greater than in women. This gender disparity has been thought to be attributable to the level of sports participation: men tend to participate more in competitive sports than women [11]. In support of this, researchers have shown that in a region where competitive netball is popular, the ratio of women with Achilles tendon ruptures was around 46% [12]. Thus, it seems that the difference in risk is not because of gender per se but because of the level of sports activity.
Etiology
Achilles tendon ruptures are generally caused by direct injury, such as through physical force on the Achilles tendon, and by concomitant degeneration of the tendon it self [13]. Although ruptures from direct injury alone rarely occur, it can occur at any site through direct trauma, crushing injury, or laceration of the posterior ankle.
The causative movements of Achilles tendon ruptures can be classified into three types: 1) most commonly, weight-bearing exerted on the extended knee as the forefoot pushes off; 2) sudden unexpected dorsiflexion of the ankle; and 3) violent dorsiflexion of the plantar flexed foot[14].
The most common site of Achilles tendon rupture is 3–6 cm proximally of the calcaneal attachment site [15], which is the site of the Achilles tendon that receives the most stress. The stress exerted in this region injures the tendon itself and can lead to degenerative changes [16].
The degenerative change is brought about as a result of a variety of factors such as chronic overloading, microtrauma, pharmacologic treatment, and heat necrosisinduced hypovascularity [17–20]. Other risk factors of Achilles tendon ruptures include age because increased collagen III and decreased collagen I with age results in less collagen cross-linking and, thus, weaker tensile
strength [20]. Further, although ischemia at the watershed region of the Achilles tendon was long thought to be causative of Achilles tendon ruptures, recent research has shown otherwise, revealing that the hemodynamic characteristics of the Achilles tendon remain unchanged during exercise and rest [21]. These tendon ruptures have been reported to be associated with oral steroid use and with intratendinous steroid injections [22]. Hypercholesterolemia, gout, rheumatoid arthritis, long-term dialysis, and kidney transplantations have also been shown to be risk factors of Achilles tendon ruptures [10].
In 2014, Claessen et al. [23] conducted a systematic review of 31 studies to investigate the predictors of Achilles tendon ruptures. Their findings show that nonmodifiable factors, such as old age, an African ethnicity, inflammation, enteritis, trauma, autoimmune arthritis, infectious arthritis, rheumatoid arthritis, tendinitis, altered collagen synthesis, and reduction in fibril size, and modifiable factors, such as obesity, use of oral Quinolone compounds and oral corticosteroids, city-dwelling, and hypercholesterolemia, exist. Of these, they found that only the reduction in fibril size was moderately associated with Achilles tendon ruptures.
Diagnosis
Clinical symptoms
Upon rupture of the Achilles tendon, patients generally experience pain in the posterior ankle as if they have been kicked from the back and hear a ‘popping’, ‘snapping’, or ‘cracking’ sound simultaneously. Patients with ruptured Achilles tendons often cannot stand on the affected leg and have reduced plantar flexion torque. Although pain usually comes instantly, some patients do not feel any pain and can walk unprohibited [24,25]. For these reasons, the patient’s visit to the hospital is often delayed, leading to either delayed or incorrect diagnosis [26].
Physical examination in patients with acute ruptures reveals odema, bruising, a palpable deficit around the rupture area, tenderness, and excess dorsiflexion of the ankle. And acute odema and bruising within 24 hours of the injury are helpful diagnostic markers in the early phase of the disease. However, with time, the deficit becomes no longer palpable because the region is filled by odema or by adipocytes. For neglected ruptures diagnosed at least 4 weeks after the injury, the deficit within the rupture is usually filled with hematoma as a result of the healing process and appears as a bulbous segment [26].
Acute Achilles tendon ruptures reduce plantar flexion torque of the ankle. The reduction in plantar flexion torque has shown to be less when the rupture lies more proximally [13]. However, active plantar flexion of the ankle is possible in spite of an Achilles tendon rupture through the compensatory actions of the flexor halluces longus, the flexor digitorum longus, the tibialis posterior, and the peroneal muscles.
An important diagnostic test for Achilles tendon ruptures is the Thompson test wherein the ability of the patient to perform plantar flexion is tested whilst the patient is laying face down, calves squeezed, and ankles on the edge of the bed. This is because an absence of plantar flexion of the ankle denotes a ruptured Achilles tendon.The sensitivity and specificity of this test was reported to be 0.96 and 0.93, respectively. However, for neglected ruptures, false negative results may appear because of partially healed tendon tissues [27,28].
In the knee flexion test, the patient lies in prone position and bends the knees 90° (which brings the tibia perpendicular to the floor). Then, the angle of the ankle is measured for both legs. A ruptured Achilles tendon is indicated by a neutral or dorsiflexed angle.
According to Maffulli [27], the sensitivity and specificity of this test is 0.88 and 0.85, respectively. According to the clinical practice guidelines developed by the American Academy of Orthopaedic Surgeons, the following diagnostic tests should be performed for Achilles tendon ruptures: a detailed medical history and two physical examinations (the Thompson test, a test for reduced plantar flexion torque, palpation of the deficit, or a test for increased passive dorsiflexion) [29]. Garras et al.[30] reported that the combination of a positive Thompson test, a positive knee flexion test, and a palpable deficit denotes a complete rupture of the Achilles tendon with a sensitivity of 100%.
Imaging evaluation
When patients show obscure clinical symptoms, diagnostic imaging should be performed using for example radiography, ultrasound, or magnetic resonance imaging (MRI) to image the axial view of the ankle (Fig. 1). In patients with Achilles tendon ruptures, an axial view of the ankle in radiological imaging would show a loss in the Kager’s triangle, the Arner sign at the distal Achilles tendon, the Toygar angle at the posterior Achilles tendon, and avulsion of the Achilles tendon attachment site[14,24].
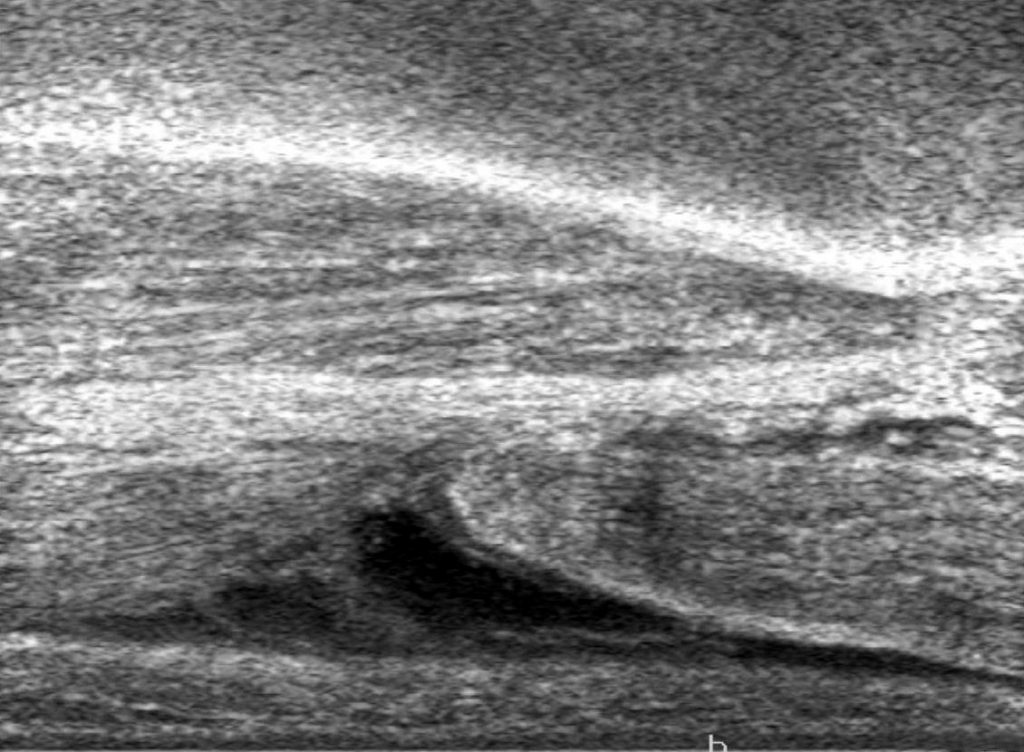
Fig. 1. An ultrasonograph shows the ruptured ends of an Achilles tendon.
Although ultrasound is a simple, cost-effective, and non-invasive method, it is heavily examiner dependent. The sensitivity of ultrasound tests has been reported to be 100%; the specificity, 89.9%; and the accuracy, 94.4% [31]. The diagnosis of Achilles tendon ruptures on ultrasound scans is be made when the deficit of the Achilles tendon is seen to be filled with fluid, debris, scar tissue, or hematoma and when dynamic imaging shows acoustic vacuum and irregular tendon ends as the patient performs plantar flexion or squeezing of the calves [31]. In dynamic imaging, the distance between the ruptured tendon ends is an important determinant of surgical treatment: some authors have suggested that a distance greater than 5 mm during plantar flexion of the foot should be an indication for surgical treatment [32,33]. In addition, ultrasound scans can be used in conservative treatment, such as cast immobilization and functional brace, to assess the position and distance of tendon ends [34].
When clinical signs do not conclusively point towards an acute Achilles tendon rupture, MRI can be used to check for soft tissue injury [24]. According to Garras et al.[30], physical examinations such as the Thompson test and the knee flexion test, which involve measuring the distance between ruptured tendon ends, show higher sensitivity for acute Achilles ruptures than MRI. For neglected ruptures, the MRI has been shown to be essential to confirm the severity of the tendon injury, to measure the distance between the ruptured tendon ends, and to determine the ideal mode of treatment [26].
Treatment
The aims of treatment in Achilles tendon ruptures are to restore the normal length and tensile strength of the Achilles tendon; to optimize its strength and function; to expedite the rehabilitation process; and to return to pre-injury levels of sports promptly. To choose the most ideal treatment for each patient, a physician must deliberate the relative benefits and complications of each treatment[35].
The treatment of Achilles tendon ruptures can be broadly divided into conservative treatment and surgical treatment. In the past, surgical treatment over non-surgical treatment had been preferred because the latter was associated with higher re-tear rates, reported to be up to 29% in some studies [36,37]. Although Lea and Smith [5] suggested that the surgical treatment of Achilles tendon ruptures is unnecessary, in 1972, only recently has the preference for non-surgical modes of treatment risen.
Conservative treatment
The conventional conservative treatment for Achilles tendon ruptures is the long-leg cast immobilization. In cast immobilization, the ankle is usually placed in 20° of plantar flexion and knee in 30° of flexion for around 2–3 weeks. Then, the plantar flexion of the ankle is incrementally decreased and either a short-leg cast or brace is administered for a three further weeks. In most cases, the patient is de-immobilization within 6–8 weeks of injury, and rehabilitation exercises are begun from active dorsiflexion of the ankle to muscle-strengthening exercises[36–38].
In the past, conservative treatment had been associated with a high re-tear rate mostly because of long-term cast immobilization. Recently, functional rehabilitation fused with conservative treatment has renewed interest in non-surgical methods for acute Achilles tendon ruptures [36,37,39]. In 1992, Saleh et al. [40] compared patients who underwent 3-weeks of cast immobilization followed by controlled early mobilization in a Sheffield splint to patients who underwent only 8-weeks of cast immobilization. They found that the former group showed significantly faster return to sports and daily activities and lower re-tear rates [40,41].
In 1995, Thermann et al. [42] suggested that as long as patients begin early weight-bearing it did not matter with respect to clinical outcomes whether patients underwent surgical treatment or conservative treatment. Also, they suggested that early cast immobilization under weight-bearing should be as short as possible and functional brace should be administered to promote weight-bearing and, therefore, to minimize muscle atrophy and stiffness. Wallace et al. [43] investigated the effectiveness of the functional brace under weight-bearing within a month of injury in 900 patients, hospitalized between 1996 and 2008, and found that only 2.8% of re-tears occurred. These findings have highlighted the advantages of conservative treatment through early joint exercise and through functional rehabilitation that gives controlled loading to the tendon. Zhang et al. [44] confirmed this through a systematic review that shows that the outcomes of conservative treatment with adjunct functional rehabilitation are comparable to those of surgical treatment in terms of the re-tear rate, the range of motion (ROM), the calf circumference, and functional outcomes. By contrast, Soroceanu et al. [45] found that those who
received conservative treatment without functional rehabilitation showed significantly higher rates of re-tear than those who received treatment with functional rehabilitation.
Surgical treatment
Direct repairs had been the preferred choice of treatment for acute Achilles tendon ruptures in the past because of their advantages of lower rates of re-tear, of favorable outcomes in terms of triceps strength recovery, and of expedited return-to-sports. But recently percutaneous and minimally invasive techniques have gained greater popularity [24,46].
Direct repairs: The direct repair of ruptured tendons minimizes the distancing of ruptured tendon ends and reduces scar tissue formation, by doing so lowering the chance of re-tears. Thus, it has long been considered as the standard treatment for Achilles tendon ruptures (Fig. 2). Direct repairs can be classified into the Krackow technique, the Bunnel technique, and the Kessler technique. Interestingly, McCoy and Haddad [47] showed that there is no treatment-dependent difference in terms of repair strength.
In a later study, Cooper [24] reported that graft or prosthesis augmentation for the repair of acute Achilles ruptures may not be always needed and recommended that the ankle should be fixed at 15°–20° of plantar flexion postoperatively to promote blood circulation of the soft tissues behind the Achilles tendon [24,48].
Percutaneous repairs: To resolve complications associated with direct repairs, Ma and Griffith [49] first suggested an alternative treatment based on percutaneous repairs in 1977. Using the percutaneous technique, they treated 18 patients under focal anesthesia and without a tourniquet and found that the length and tensile strength of the Achilles tendon were restored with minimal post-operative complications and without any iatrogenic sural nerve injuries. Conversely, Klein et al. [50] observed sural nerve damage in 13% of patients with Achilles tendon ruptures when they used the Ma and Griffith’s technique [49]. In a comparative study, percutaenous repair was found to be superior to direct repairs in terms of re-tear rate, aesthetic appearance, and postoperative complications, such as infections [51]. However, percutaneous re-
pairs have been shown to be associated with higher rates of sciatic nerve injuries [52].
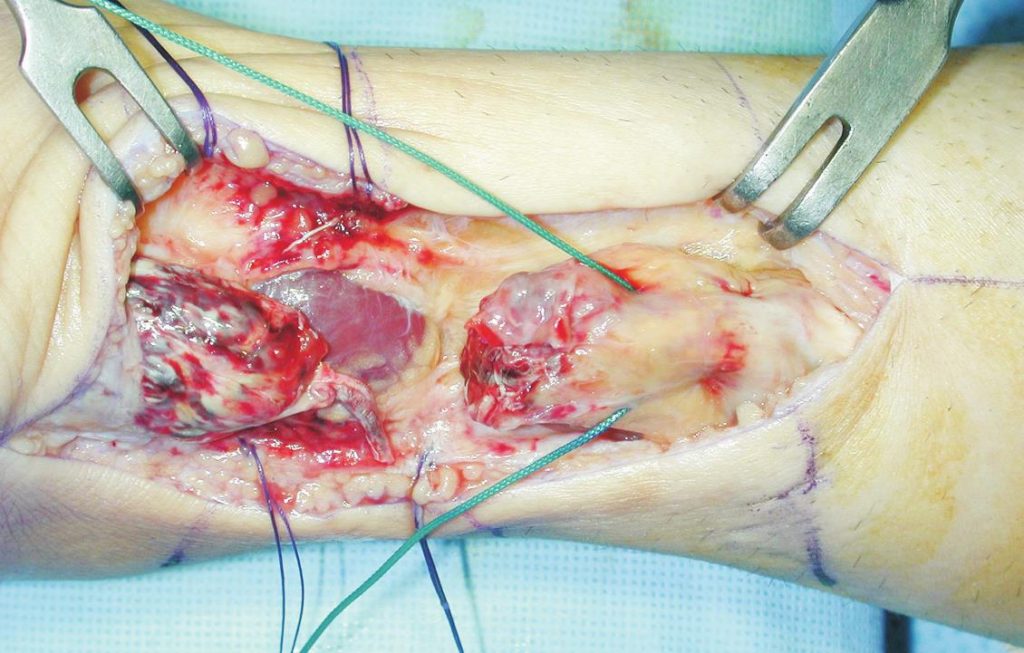
Fig. 2. An intraoperative photograph shows a ruptured Achilles tendon and a non-absorbable suture that was passed through the proximal end using the Bunnel technique.
Mini-open repairs: Greater interest in the anatomical course of the sural nerve was sparked by research by Klein et al.’s group [50]. A cadaveric study reported that at the level at which the sural nerve inserts into the calcaneus of the Achilles tendon, the sural nerve crosses the lateral border on average 18.8 mm anterolateral of the lateral border and 9.8 cm from the calcaneus [53]. On the basis of this finding, Webb and Bannister [54] developed a novel minimal incision technique which involves making three stab incisions along the posterior mid-section of the Achilles tendon and performing an approximation of the tendon. To approximate the tendon ends, two box stitches are made using a 90-mm cutting needle and a No. 1 nylon suture.
In 2002, Assal et al. [55] conducted a limited open repair using the newly developed Achillon device (Integra Life-Sciences, Plainsboro, NJ, USA), which places the suture in the paratenon in order to minimize sural nerve injury. However, a disadvantage of this technique is that it cannot prevent needle-related damages.
The purpose of such mini-open repairs is to lower the re-tear rate as in direct repairs, as well as reducing soft tissue infections. Yet complications such as sural nerve entrapment, skin adherence, unreliable tendon apposition, and weak repair strength still remain [56].
Postoperative rehabilitation
Previously, Brumann et al. [57] conducted a systematic review to develop an evidence-based postoperative protocol. They found that compared to the non–weight-bearing group the full weight-bearing group was associated with a quicker return to gait and to pre-injury levels of sports and with significantly better patient satisfaction. Further, they found that the group that performed joint exercises returned to sports or to work faster than the group that did not perform joint exercises. These observations have led to the recommendation of the following protocol [57]:
- Administer a postoperative splint or brace under full weight-bearing in 30° of plantar flexion of the ankle.
- Begin joint exercises from the third postoperative week and reduce plantar flexion angle by 10° every week until an angle of 0° is reached. Allow weight-bearing without brace from the 7th postoperative week.
- Begin rehabilitation to increase muscle strength, ROM, and proprioception.
The protocol indicates that early joint exercise and weight-bearing are regarded as important adjunct treatments for both surgical and non-surgical treatments.
CONCLUSION
With an ever increasing active population, the incidence of Achilles tendon ruptures is set to rise even further. Although several treatment methods both conservative and surgical (direct repairs, percutaneous repairs, and mini-open repairs) exist, a standardized gold-standard treatment has not been established. Thus, further studies are required to investigate the best treatment for Achilles tendon ruptures that minimizes complications, such as re-tears, muscle weakening, skin-related disorders, and sciatic nerve injuries.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
- Thompson J, Baravarian B. Acute and chronic Achilles tendon ruptures in athletes. Clin Podiatr Med Surg 2011;28:117-35.
- Maquirriain J. Achilles tendon rupture: avoiding tendon lengthening during surgical repair and rehabilitation. Yale J Biol Med 2011;84:289-300.
- Gulati V, Jaggard M, Al-Nammari SS, et al. Management of Achilles tendon injury: a current concepts systematic review. World J Orthop 2015;6:380-6.
- Parekh SG, Wray WH 3rd, Brimmo O, Sennett BJ, Wapner KL. Epidemiology and outcomes of Achilles tendon ruptures in the National Football League. Foot Ankle Spec 2009;2:283-6.
- Lea RB, Smith L. Non-surgical treatment of tendo Achillis rupture. J Bone Joint Surg Am 1972;54:1398-407.
- Möller A, Astron M, Westlin N. Increasing incidence of Achilles tendon rupture. Acta Orthop Scand 1996;67:479-81.
- Nyyssönen T, Lüthje P, Kröger H. The increasing incidence and difference in sex distribution of Achilles tendon rupture in Finland in 1987-1999. Scand J Surg 2008;97:272-5.
- Nillius SA, Nilsson BE, Westlin NE. The incidence of Achilles tendon rupture. Acta Orthop Scand 1976;47:118-21.
- Maffulli N, Waterston SW, Squair J, Reaper J, Douglas AS. Changing incidence of Achilles tendon rupture in Scotland: a 15-year study. Clin J Sport Med 1999;9:157-60.
- Sode J, Obel N, Hallas J, Lassen A. Use of fluroquinolone and risk of Achilles tendon rupture: a population-based cohort study. Eur J Clin Pharmacol 2007;63:499-503.
- Movin T, Ryberg A, McBride DJ, Maffulli N. Acute rupture of the Achilles tendon. Foot Ankle Clin 2005;10:331-56.
- Gwynne-Jones DP, Sims M, Handcock D. Epidemiology and out-comes of acute Achilles tendon rupture with operative or nonoperative treatment using an identical functional bracing protocol. Foot Ankle Int 2011;32:337-43.
- Coughlin MJ, Saltzman CL, Anderson RB. Mann’s surgery of the foot and ankle. 9th ed. Philadelpia, PA: Elsevier; 2014.
- Arner O, Lindholm A, Orell SR. Histologic changes in subcutaneous rupture of the Achilles tendon; a study of 74 cases. Acta Chir Scand 1959;116:484-90.
- Flik KR, Bush-Joseph CA, Bach BR Jr. Complete rupture of large tendons: risk factors, signs, and definitive treatment. Phys Sportsmed 2005;33:19-28.
- Barfred T. Experimental rupture of the Achilles tendon. Comparison of various types of experimental rupture in rats. Acta Orthop Scand 1971;42:528-43.
- Ahmed IM, Lagopoulos M, McConnell P, Soames RW, Sefton GK. Blood supply of the Achilles tendon. J Orthop Res 1998;16:591-6.
- Bernard-Beaubois K, Hecquet C, Hayem G, Rat P, Adolphe M. In vitro study of cytotoxicity of quinolones on rabbit tenocytes. Cell Biol Toxicol 1998;14:283-92.
- Maffulli N, Longo UG, Maffulli GD, Rabitti C, Khanna A, Denaro V. Marked pathological changes proximal and distal to the site of rupture in acute Achilles tendon ruptures. Knee Surg Sports Traumatol Arthrosc 2011;19:680-7.
- Maffulli N, Ewen SW, Waterston SW, Reaper J, Barrass V. Tenocytes from ruptured and tendinopathic Achilles tendons produce greater quantities of type III collagen than tenocytes from normal Achilles tendons. An in vitro model of human tendon healing. Am J Sports Med 2000;28:499-505.
- Komi PV, Fukashiro S, Järvinen M. Biomechanical loading of Achilles tendon during normal locomotion. Clin Sports Med 1992;11:521-31.
- Newnham DM, Douglas JG, Legge JS, Friend JA. Achilles tendon rupture: an underrated complication of corticosteroid treatment. Thorax 1991;46:853-4.
- Claessen FM, de Vos RJ, Reijman M, Meuffels DE. Predictors of primary Achilles tendon ruptures. Sports Med 2014;44:1241-59.
- Cooper MT. Acute Achilles tendon ruptures: does surgery offer superior results (and other confusing issues)? Clin Sports Med 2015;34:595-606.
- Leppilahti J, Orava S. Total Achilles tendon rupture. A review. Sports Med 1998;25:79-100.
- Bevilacqua NJ. Treatment of the neglected Achilles tendon rupture. Clin Podiatr Med Surg 2012;29:291-9, viii.
- Maffulli N. The clinical diagnosis of subcutaneous tear of the Achilles tendon. A prospective study in 174 patients. Am J Sports Med 1998;26:266-70.
- Thompson TC. A test for rupture of the tendo Achillis. Acta Orthop Scand 1962;32:461-5.
- Chiodo CP, Glazebrook M, Bluman EM, et al. American Academy of Orthopaedic Surgeons clinical practice guideline on treatment of Achilles tendon rupture. J Bone Joint Surg Am 2010;92:2466-8.
- Garras DN, Raikin SM, Bhat SB, Taweel N, Karanjia H. MRI is unnecessary for diagnosing acute Achilles tendon ruptures: clinical diagnostic criteria. Clin Orthop Relat Res 2012;470:2268-73.
- Rockett MS, Waitches G, Sudakoff G, Brage M. Use of ultrasonography versus magnetic resonance imaging for tendon abnormalities around the ankle. Foot Ankle Int 1998;19:604-12.
- Margetić P, Miklić D, Rakić-Ersek V, Doko Z, Lubina ZI, Brkljacić B. Comparison of ultrasonographic and intraoperative findings in Achilles tendon rupture. Coll Antropol 2007;31:279-84.
- Kotnis R, David S, Handley R, Willett K, Ostlere S. Dynamic ultra-sound as a selection tool for reducing Achilles tendon reruptures. Am J Sports Med 2006;34:1395-400.
- Kauwe M. Acute Achilles tendon rupture: clinical evaluation, conservative management, and early active rehabilitation. Clin Podiatr Med Surg 2017;34:229-43.
- Thevendran G, Sarraf KM, Patel NK, Sadri A, Rosenfeld P. The ruptured Achilles tendon: a current overview from biology of rupture to treatment. Musculoskelet Surg 2013;97:9-20.
- Möller M, Movin T, Granhed H, Lind K, Faxén E, Karlsson J. Acute rupture of tendon Achillis. A prospective randomised study of comparison between surgical and non-surgical treatment. J Bone Joint Surg Br 2001;83:843-8.
- Inglis AE, Scott WN, Sculco TP, Patterson AH. Ruptures of the tendon Achillis. An objective assessment of surgical and non-surgical treatment. J Bone Joint Surg Am 1976;58:990-3.
- Kim YJ, Ahn JH, Shin DC. Conservative treatment of Achilles tendon rupture with ultrasonographic follow-up: a case report. J Korean Orthop US Soc 2011;4:88-92.
- Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U. Operative versus nonoperative treatment of Achilles tendon rupture. A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-9.
- Saleh M, Marshall PD, Senior R, MacFarlane A. The Sheffield splint for controlled early mobilisation after rupture of the calcaneal tendon. A prospective, randomised comparison with plaster treatment. J Bone Joint Surg Br 1992;74:206-9.
- Huttunen TT, Kannus P, Rolf C, Felländer-Tsai L, Mattila VM. Acute Achilles tendon ruptures: incidence of injury and surgery in Sweden between 2001 and 2012. Am J Sports Med 2014;42:2419-23.
- Thermann H, Zwipp H, Tscherne H. Functional treatment concept of acute rupture of the Achilles tendon. 2 years results of a prospective randomized study. Unfallchirurg 1995;98:21-32.
- Wallace RG, Heyes GJ, Michael AL. The non-operative functional management of patients with a rupture of the tendo Achillis leads to low rates of re-rupture. J Bone Joint Surg Br 2011;93:
1362-6.
- Zhang H, Tang H, He Q, et al. Surgical versus conservative intervention for acute Achilles tendon rupture: a prisma-compliant systematic review of overlapping meta-analyses. Medicine (Baltimore) 2015;94:e1951.
- Soroceanu A, Sidhwa F, Aarabi S, Kaufman A, Glazebrook M. Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials. J Bone Joint Surg Am 2012;94:2136-43.
- Yang B, Liu Y, Kan S, et al. Outcomes and complications of percutaneous versus open repair of acute Achilles tendon rupture: a meta-analysis. Int J Surg 2017;40:178-86.
- McCoy BW, Haddad SL. The strength of Achilles tendon repair: a comparison of three suture techniques in human cadaver tendons. Foot Ankle Int 2010;31:701-5.
- Pajala A, Kangas J, Siira P, Ohtonen P, Leppilahti J. Augmented compared with nonaugmented surgical repair of a fresh total Achilles tendon rupture. A prospective randomized study. J Bone
Joint Surg Am 2009;91:1092-100.
- Ma GW, Griffith TG. Percutaneous repair of acute closed ruptured Achilles tendon: a new technique. Clin Orthop Relat Res 1977;(128):247-55.
- Klein W, Lang DM, Saleh M. The use of the Ma-Griffith technique for percutaneous repair of fresh ruptured tendo Achillis. Chir Organi Mov 1991;76:223-8.
- Khan RJ, Fick D, Keogh A, Crawford J, Brammar T, Parker M. Treatment of acute Achilles tendon ruptures. A meta-analysis of randomized, controlled trials. J Bone Joint Surg Am 2005;87:
2202-10.
- Wilkins R, Bisson LJ. Operative versus nonoperative management of acute Achilles tendon ruptures: a quantitative systematic review of randomized controlled trials. Am J Sports Med 2012;40:2154-60.
- Webb J, Moorjani N, Radford M. Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-7.
- Webb JM, Bannister GC. Percutaneous repair of the ruptured tendo Achillis. J Bone Joint Surg Br 1999;81:877-80.
- Assal M, Jung M, Stern R, Rippstein P, Delmi M, Hoffmeyer P. Limited open repair of Achilles tendon ruptures: a technique with a new instrument and findings of a prospective multicenter
study. J Bone Joint Surg Am 2002;84:161-70.
- Davies MS, Solan M. Minimal incision techniques for acute Achilles repair. Foot Ankle Clin 2009;14:685-97.
- Brumann M, Baumbach SF, Mutschler W, Polzer H. Accelerated rehabilitation following Achilles tendon repair after acute rupture: development of an evidence-based treatment protocol. Injury 2014;45:1782-90.

